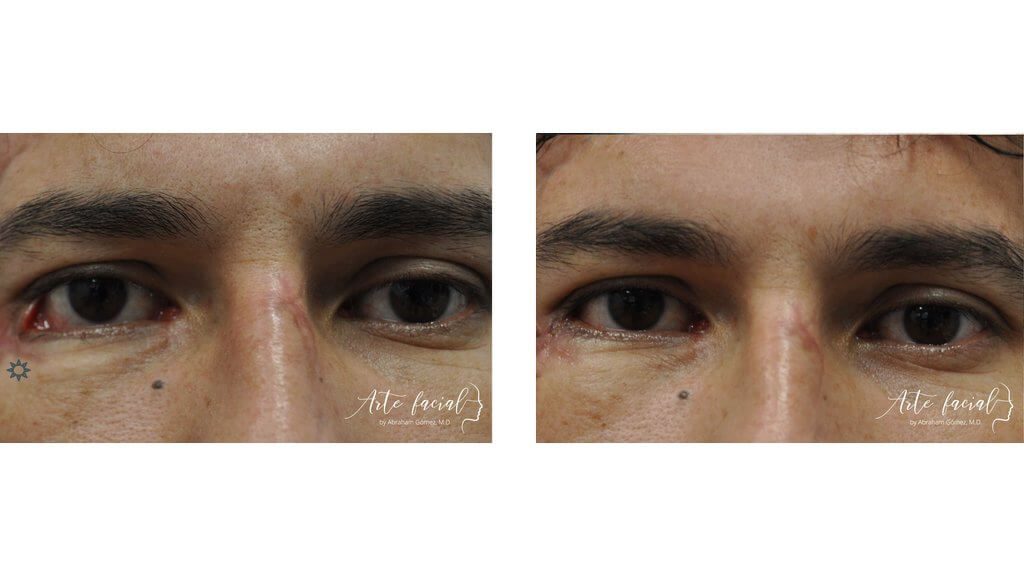
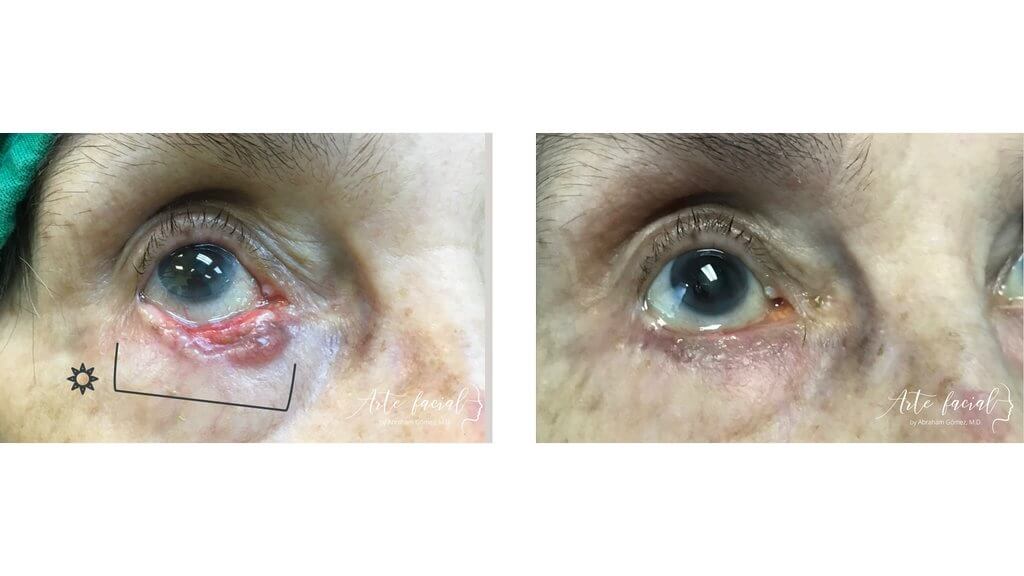
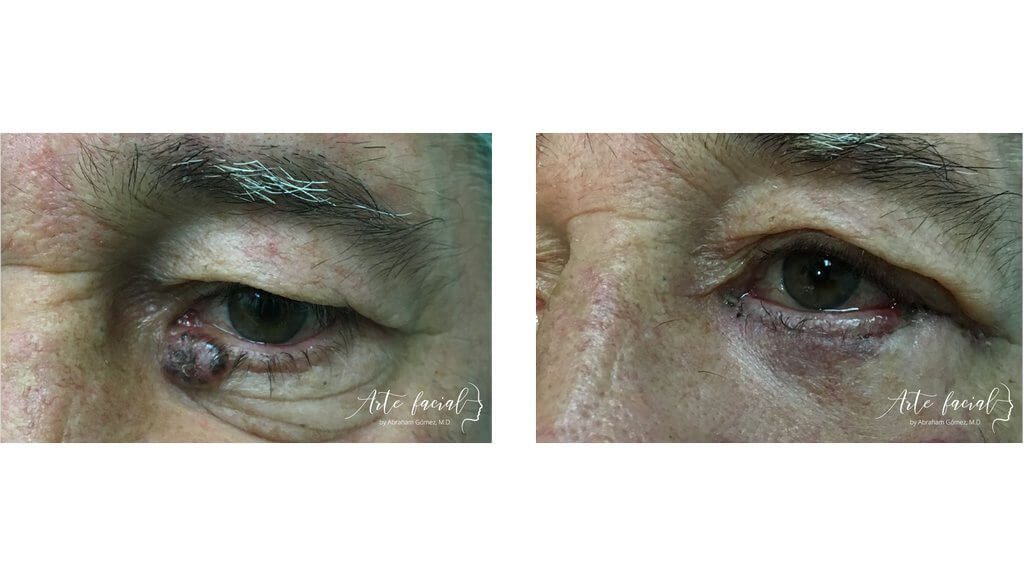
Before
After
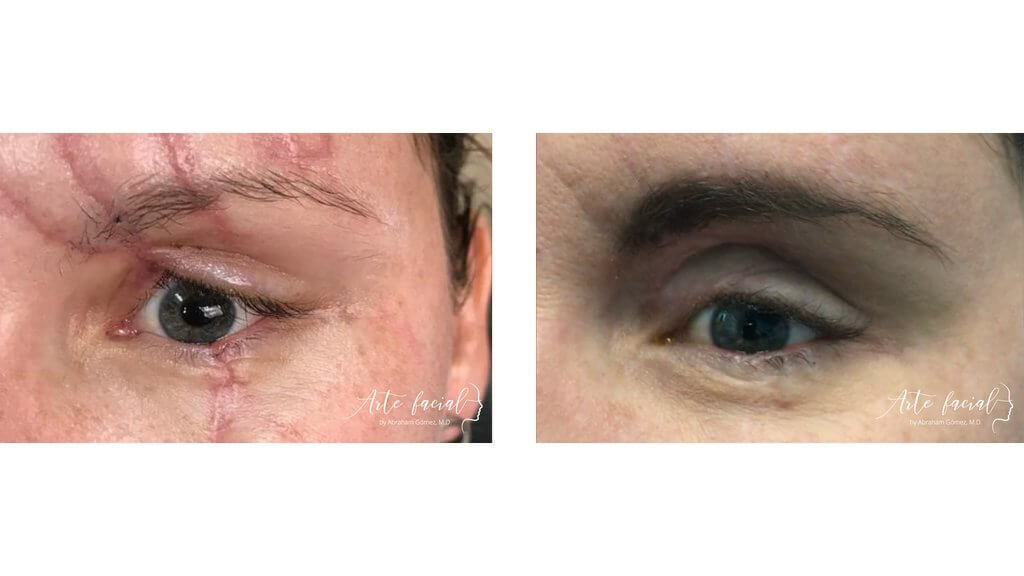

An orbital fracture occurs when acute trauma to the eye causes a rupture of one or several bony walls in the eye socket. The paper-thin orbital floor and medial walls are especially vulnerable to rupture due to blunt force trauma, from a tennis ball to a fist or an accidental kick from a horse.
The orbital surgeon must carefully approach the evaluation and subsequent management of a fracture since not all orbital fractures require surgical intervention. If the management is surgical, the surgeon may desire to allow some time for the orbital swelling to improve before proceeding with the operation. Also, pediatric orbital fractures require different surgical timelines from adult ones.
These and other factors warrant an organized evaluation and careful thought process on behalf of the orbital surgeon to minimize long-term sequelae and obtain the best functional and cosmetic outcome.
An orbital brow-out fracture happens when direct, blunt force is applied to the orbit, as from a fall, vehicle accident, or fist strike. In these cases, the force is transmitted to the walls of the orbit. The lateral wall and roof of the orbit can withstand a strong force without suffering significant damage; however, the floor and medial wall are so thin that they can fracture with relative ease.
The clinical symptoms of an orbital blow-out fracture will vary as it depends on several factors such as the extent of the fracture, mechanism of trauma, the severity of tissue damage, and the patient’s age.
A minor orbital floor fracture may be asymptomatic, and patients may complain of only mild discomfort. On the other hand, large fractures involving the floor and medial wall may cause multiple symptoms, such as nausea, loss of sensation on the cheek, and double vision. The eye may also be pushed back into the orbit (enophthalmos) or be displaced downward (hypoglobus).
An orbital blow-out fracture does not always require surgery, and in fact, a significant percentage of fractures in adults only need to be observed. It is essential to be cautious when deciding to operate because the procedure carries significant risk. Complications of this surgery may include permanent cheek numbness, scarring of the lower eyelid, worsening of double vision, and even permanent vision loss. Therefore, the decision to operate must be derived from evidence-based medicine rather than empirical knowledge.
The indications for operating an orbital blow-out fracture include:
The first and most crucial step in repairing an orbital blow-out fracture is waiting for the swelling to subside before surgery. Operating a fracture on a swollen orbit can make the operation more complex and produce a less predictable result. The exception is in cases involving children, where a blow-out fracture may require urgent repair.
The operation is performed under general anesthesia. The preferred method for entering the orbit is through an incision on the inside of the eyelid (transconjunctival) rather than through the skin (transcutaneous approach). Dissection is carried out between the globe and the orbit until reaching the fracture. Then, the surgeon identifies the location and extent of the fracture and elevates the tissues that are entrapped inside the bony defect. Lastly, an implant made of titanium or other material is placed over the fracture and fixated to the bone around the fracture.
The patient stays in the hospital for one night for observation.
Before
After

+506 7032-5570
Abraham Gómez, MD
Hospital Clínica Bíblica, Omega Building, 2nd floor
Loras Medical, Torre Las Loras, main floor
+506 7032-5570
Abraham Gómez, MD
Hospital Clínica Bíblica, Omega Building, 2nd floor
Loras Medical, Torre Las Loras, main floor
ARTE FACIAL
ARTE FACIAL

Visit us at our new office! 25% off on your consultation at Loras Medical. Book here (Valid Until December 15, 2023.)
Please fill out the form below to schedule a virtual consultation with Dr. Gomez.
 |
|